If you're a nursing student preparing for your nursing license exam , you know how important it is to have access to high-quality study materials.
Sample case study for nursing students can be a valuable tool in your preparation, helping you to develop critical thinking skills and apply your knowledge in real-world scenarios.
That's why we've put together a list of 5 nursing case study examples, complete with answer guides, to help you prepare for the NCLEX-style questions you'll encounter on exam day.
Mrs. Johnson is a 62-year-old female who was admitted to the hospital with a complaint of severe headache and dizziness. She has a past medical history of hypertension for the past 5 years, and she has been on antihypertensive medications.
She has a family history of hypertension and heart disease, with her mother and brother both diagnosed with hypertension. Mrs. Johnson is currently working as a school teacher and lives with her husband. She has a sedentary lifestyle and reports occasional non-adherence to her medications due to forgetfulness.
Upon admission, Mrs. Johnson's vital signs are as follows: blood pressure (BP) 180/100 mmHg, heart rate (HR) 88 beats per minute (BPM), respiratory rate (RR) 18 breaths per minute, and temperature 98.6°F.
She is alert and oriented but complains of a throbbing headache and lightheadedness. Her skin is warm and dry, and there is no visible edema. Her lungs are clear on auscultation, and her heart sounds are normal with no murmurs. Her abdominal assessment reveals no tenderness or masses. Mrs. Johnson's laboratory results show an elevated fasting blood glucose level of 135 mg/dL, cholesterol level of 240 mg/dL, and serum creatinine level of 1.2 mg/dL. She has a body mass index (BMI) of 30, which indicates obesity.
1. What are the risk factors for hypertension in this case study?
2. What are the signs and symptoms of hypertension in Mrs. Johnson?
3. What other assessments should the nurse prioritize for Mrs. Johnson?
4. What nursing interventions would be appropriate for Mrs. Johnson's hypertension management?
5. What patient education should the nurse provide to Mrs. Johnson regarding hypertension management?
6. What referrals or consultations should the nurse consider for Mrs. Johnson?
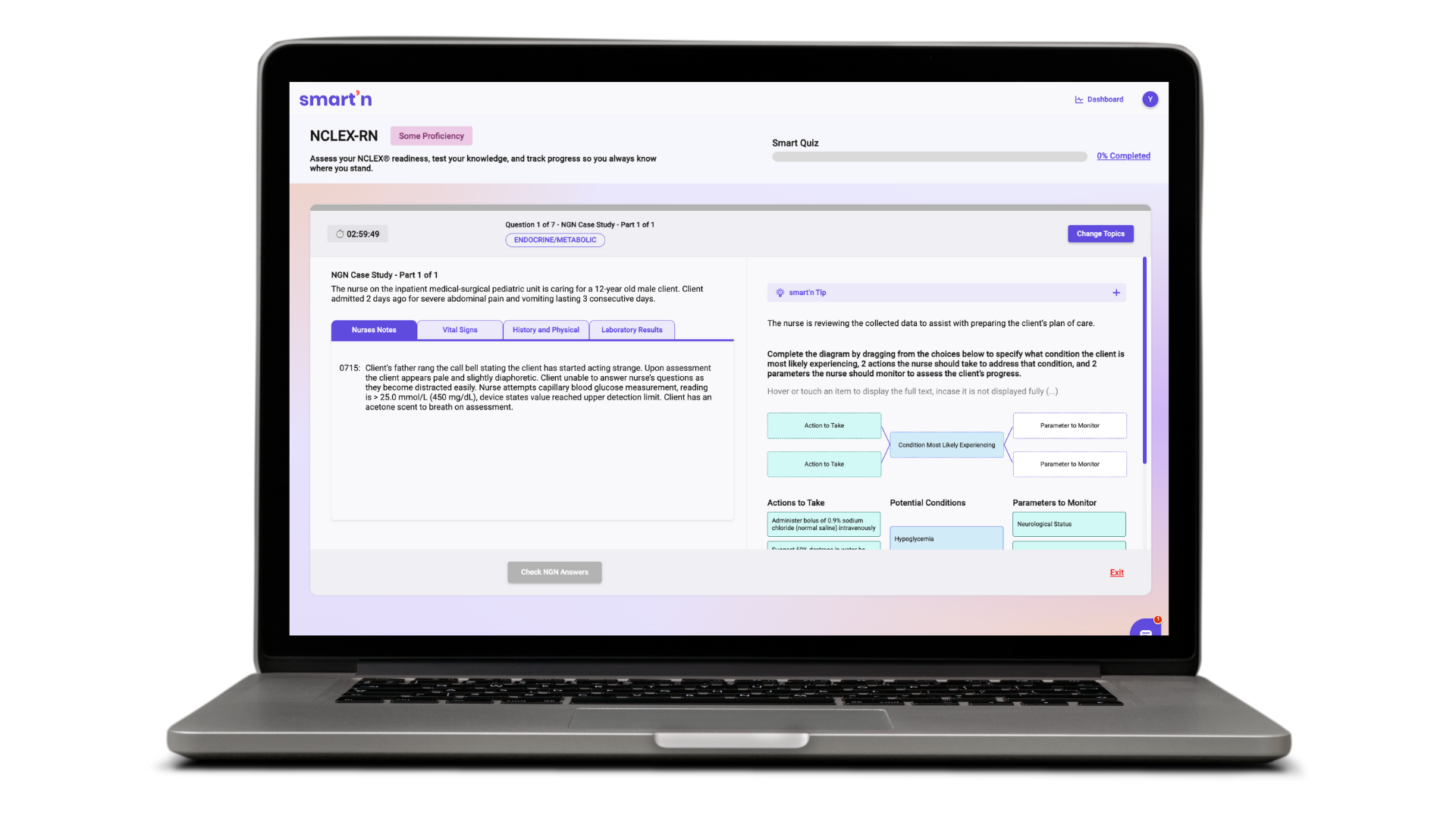
Experience AI-enabled learning support for nurses on Smart ’ n.
Mr. Thompson is a 68-year-old male with a history of type 2 diabetes for the past 15 years. He has a sedentary lifestyle and a BMI of 32, indicating obesity. Mr. Thompson has a history of poor glycemic control with frequent episodes of hyperglycemia and occasional non-adherence to his diabetic medications due to financial constraints.
He presents to the clinic with a complaint of a non-healing ulcer on his right foot for the past 2 weeks. He reports that he accidentally bumped his foot against a hard object and developed a small blister that has since progressed to a deep, painful ulcer with foul-smelling drainage.
Upon assessment, Mr. Thompson's vital signs are stable with a blood pressure (BP) of 132/82 mmHg, heart rate (HR) of 76 beats per minute (BPM), respiratory rate (RR) of 18 breaths per minute, and temperature of 98.2°F.
He appears anxious and in mild distress due to the pain from the foot ulcer. His right foot is swollen, erythematous, and warm to the touch, with a deep, irregularly-shaped ulcer measuring approximately 3 cm x 4 cm on the plantar surface.
There is purulent drainage with a foul odor, and the surrounding skin is macerated. Mr. Thompson has diminished sensation in his right foot and a weak dorsalis pedis pulse. His laboratory results show an elevated fasting blood glucose level of 240 mg/dL and a hemoglobin A1c level of 9.5%.
1. What are the risk factors for the development of diabetic foot ulcer in Mr. Thompson?
2. What are the signs and symptoms of the diabetic foot ulcer in Mr. Thompson?
3. What other assessments should the nurse prioritize for Mr. Thompson's diabetic foot ulcer management?
4. What nursing interventions would be appropriate for Mr. Thompson's diabetic foot ulcer management?
5. What patient education should the nurse provide to Mr. Thompson regarding diabetic foot ulcer management?
6. What interdisciplinary team members may be involved in Mr. Thompson's diabetic foot ulcer management?
Mich is a 15-year-old male who was brought to the emergency department by his parents due to complaints of chest pain and shortness of breath. Mich has a history of asthma and had been experiencing symptoms for the past two days. Mich's parents reported that he had been compliant with his asthma medications but had recently run out of his inhaler. Upon arrival at the emergency department, Mich was found to have a rapid heart rate and was diagnosed with a severe asthma exacerbation.
On assessment, Mich appeared anxious and in distress, with labored breathing and a respiratory rate of 30 breaths per minute. His oxygen saturation was 88% on room air, and he was immediately started on supplemental oxygen via nasal cannula.
Mich's chest exam was significant for decreased breath sounds and wheezing. His heart rate was 130 beats per minute, and his blood pressure was 120/70 mmHg. Mich's laboratory values were within normal limits, except for an elevated white blood cell count, which was likely due to his asthma exacerbation.
1. What is the priority nursing intervention for Mich?
The priority nursing intervention for Mich is to assess and manage his respiratory distress. This includes providing supplemental oxygen, administering bronchodilator medications, and monitoring his response to treatment.
2. What education should the nurse provide to Mich and his parents?
The nurse should educate Mich and his parents on the proper use of asthma medications, including inhalers and nebulizers. The nurse should also provide education on asthma triggers and how to avoid them, as well as signs and symptoms of an asthma exacerbation and when to seek medical attention.
3. What potential complications should the nurse monitor for in Mich?
The nurse should monitor Mich for potential complications of asthma exacerbation, including respiratory failure, pneumothorax, and cardiac complications such as arrhythmias. The nurse should also monitor for signs of anxiety and provide emotional support to Mich and his family.
4. How can the nurse promote adherence to Mich's asthma treatment regimen?
The nurse can promote adherence to Mich's asthma treatment regimen by providing education and resources, such as written instructions and referrals to support groups. The nurse can also encourage open communication with Mich and his family and address any barriers to adherence, such as cost or access to medications.
5. What discharge planning should the nurse initiate for Mich?
The nurse should initiate discharge planning that includes instructions for Mich and his family on proper asthma management at home. This includes providing education on medication administration, recognizing signs and symptoms of asthma exacerbation, and developing an asthma action plan. The nurse should also ensure that Mich has access to his medications and any necessary equipment, such as a peak flow meter or spacer. Referral to a primary care provider or asthma specialist for ongoing management should also be initiated. Finally, the nurse should provide education on follow-up appointments and any necessary referrals for additional support services, such as social work or mental health resources.
6. How can the nurse promote family-centered care for Mich and his parents?
The nurse can promote family-centered care by involving Mich and his parents in the care planning process and encouraging their participation in decision-making. The nurse can provide emotional support and education to help them feel confident in their role as caregivers, and address any cultural or religious needs of the family to promote a holistic approach to care. The nurse should also encourage family visitation and provide opportunities for Mich and his parents to ask questions and express concerns.
Baby S is a 10-day-old infant who was admitted to the neonatal intensive care unit (NICU) due to respiratory distress and hypoxemia. Baby S was born prematurely at 34 weeks gestation via emergency cesarean section due to fetal distress.
The mother had a history of preeclampsia and received antenatal corticosteroids. Baby S had a birth weight of 2.2 kg and required immediate intubation and mechanical ventilation.
On assessment, Baby S appeared to be in moderate respiratory distress, with a respiratory rate of 50 breaths per minute, nasal flaring, and intercostal retractions. Her oxygen saturation was 88% on a fraction of inspired oxygen (FiO2) of 0.5, and her heart rate was 160 beats per minute. Lung auscultation revealed bilateral crackles, and the chest X-ray showed diffuse bilateral infiltrates consistent with respiratory distress syndrome (RDS). Baby S had a central line for parenteral nutrition and was receiving intravenous fluids and medications.
1. What is the pathophysiology of RDS in premature infants?
RDS is a common respiratory disorder in premature infants, caused by a deficiency of pulmonary surfactant, which normally keeps the alveoli open and prevents collapse. In premature infants, the lungs are not fully developed, and surfactant production is inadequate, leading to increased surface tension and collapse of the alveoli. This results in ventilation-perfusion (V/Q) mismatch, hypoxemia, and respiratory distress.
2. What interventions should the nurse implement for Baby S?
The nurse should ensure that Baby S is receiving appropriate respiratory support, including mechanical ventilation, FiO2 titration, and positive end-expiratory pressure (PEEP) as prescribed. The nurse should also monitor Baby S's vital signs, oxygen saturation, and blood gas values closely to optimize oxygenation and ventilation. The nurse should maintain a sterile environment around the central line and monitor for signs of infection. The nurse should also provide enteral or parenteral nutrition as prescribed to meet the infant's metabolic needs and promote growth.
3. What potential complications should the nurse monitor for in Baby S?
The nurse should monitor for potential complications such as infection, barotrauma, bronchopulmonary dysplasia (BPD), and patent ductus arteriosus (PDA). Infection is a common complication in premature infants and can be life-threatening. Barotrauma can occur due to excessive mechanical ventilation and can result in pneumothorax or other complications. BPD is a chronic lung disease that can develop in premature infants who require prolonged mechanical ventilation or oxygen therapy. PDA is a common cardiac complication in premature infants, resulting in abnormal blood flow between the aorta and pulmonary artery.
4. How can the nurse support Baby S's developmental care needs?
The nurse can support Baby S's developmental care needs by providing a quiet and dark environment, minimizing unnecessary handling and stimulation, and promoting restful sleep. The nurse can also encourage skin-to-skin contact with the mother or father to promote bonding and provide comfort. The nurse should also provide appropriate pain management for any procedures or interventions to minimize discomfort and stress.
5. What discharge planning should the nurse initiate for Baby S?
The nurse should initiate discharge planning as early as possible to ensure a smooth transition to home. The nurse should provide education to the parents about the infant's medical needs, including respiratory support, feeding, medication administration, and infection prevention. The nurse should also refer the parents to appropriate community resources, such as home health services, support groups, and developmental follow-up clinics. The nurse should work with the healthcare team to develop a plan for ongoing monitoring and follow-up to ensure that Baby S's medical needs are being met and to monitor for any potential complications or developmental delays.
6. How can the nurse promote family-centered care for Baby S and her parents?
The nurse can do so by involving the parents in the infant's care as much as possible, encouraging their participation in decision-making, and providing emotional support and education to help them feel confident in their role as caregivers. The nurse can also encourage family visitation and provide opportunities for parent-infant bonding, such as skin-to-skin contact and feeding. The nurse should also recognize and address any cultural or religious needs of the family to promote a holistic approach to care.
Mrs. Jones is a 72-year-old female who underwent total hip replacement surgery due to severe hip osteoarthritis. She has a history of hypertension and osteoporosis. Mrs. Jones lives alone and has limited mobility due to hip pain and stiffness prior to surgery. She was admitted to the orthopedic surgical unit and is now postoperative day 1 after her surgery.
1. What are the priority nursing diagnoses for Mrs. Jones?
2. What are the nursing interventions to address Mrs. Jones's acute pain?
3. How can the nursing team assist Mrs. Jones with impaired physical mobility?
4. What nursing interventions can be implemented to prevent infection in Mrs. Jones?
5. What should be included in Mrs. Jones's education and discharge planning?
6. How will the nursing team evaluate the effectiveness of the care provided to Mrs. Jones?
Experience AI-enabled learning support for nurses on Smart ’ n.