- Non–ST-segment elevation
- ST-segment elevation
- Prinzmetal variant
- Stable
- Unstable
- Essential hypertension
- Hypertensive emergencies
- Secondary hypertension
- Cardiogenic shock
- Orthostatic hypotension
- Vasovagal hypotension
- Hypercholesterolemia
- Hypertriglyceridemia
Traumatic, infectious, and inflammatory heart conditions
- Acute and subacute bacterial endocarditis
- Acute pericarditis
- Cardiac tamponade
- Pericardial effusion
- Aortic aneurysm/dissection
- Arterial embolism/thrombosis
- Arteriovenous malformation
- Giant cell arteritis
- Peripheral artery disease
- Phlebitis/thrombophlebitis
- Varicose veins
- Venous insufficiency
- Venous thrombosis
- Acne vulgaris
- Folliculitis
- Rosacea
- Erythema multiforme
- Stevens-Johnson syndrome
- Toxic epidermal necrolysis
Diseases/disorders of the hair and nails
- Alopecia
- Onychomycosis
- Paronychia
Envenomations and arthropod bite reactions
- Erythema infectiosum (fifth disease)
- Hand-foot-and-mouth disease
- Measles
- Bacterial
- Cellulitis
- Erysipelas
- Impetigo
- Candidiasis
- Dermatophyte infections
- Lice
- Scabies
- Condyloma acuminatum
- Herpes simplex
- Molluscum contagiosum
- Varicella-zoster virus infections
- Verrucae
- Actinic keratosis
- Seborrheic keratosis
- Benign
- Malignant
- Premalignant
- Contact dermatitis
- Drug eruptions
- Eczema
- Lichen planus
- Pityriasis rosea
- Psoriasis
- Burns
- Lacerations
- Pressure ulcers
- Stasis dermatitis
- Cherry angioma
- Telangiectasia
Other dermatologic disorders
- Acanthosis nigricans
- Hidradenitis suppurativa
- Lipomas/epidermal inclusion cysts
- Photosensitivity reactions
- Pilonidal disease
- Urticaria
- Primary adrenal insufficiency
- Cushing syndrome
- Multiple endocrine neoplasia
- Neoplastic syndrome
- Primary endocrine malignancy
- Syndrome of inappropriate antidiuretic hormone secretion (SIADH)
- Hyperparathyroidism
- Hypoparathyroidism
- Acromegaly/gigantism
- Diabetes insipidus
- Dwarfism
- Pituitary adenoma
- Hyperthyroidism
- Hypothyroidism
- Thyroiditis
- Conjunctival disorders
- Conjunctivitis
- Cataract
- Corneal ulcer
- Infectious
- Keratitis
- Pterygium
- Dacryocystitis
- Blepharitis
- Chalazion
- Ectropion
- Entropion
- Hordeolum
- Nystagmus
- Optic neuritis
- Papilledema
- Orbital cellulitis
- Macular degeneration
- Retinal detachment
- Retinopathy
- Blowout fracture
- Corneal abrasion
- Globe rupture
- Hyphema
- Retinal vascular occlusion
- Amaurosis fugax
- Amblyopia
- Glaucoma
- Scleritis
- Strabismus
- External ear
- Cerumen impaction
- Otitis externa
- Trauma
- Acoustic neuroma
- Barotrauma
- Dysfunction of eustachian tube
- Labyrinthitis
- Vertigo
- Cholesteatoma
- Otitis media
- Tympanic membrane perforation
Other abnormalities of the ear
- Mastoiditis
- Meniere disease
- Tinnitus
- Epistaxis
- Nasal polyps
- Rhinitis
- Sinusitis
- Trauma
- Diseases of the teeth/gums
- Infectious/inflammatory disorders
- Aphthous ulcers
- Candidiasis
- Deep neck infection
- Epiglottitis
- Herpes simplex
- Laryngitis
- Peritonsillar abscess
- Pharyngitis
- Sialadenitis
- Parotitis
- Leukoplakia
- Acute/chronic cholecystitis
- Cholangitis
- Cholelithiasis
- Abscess/fistula
- Anal fissure
- Constipation
- Diverticulitis
- Fecal impaction
- Hemorrhoids
- Inflammatory bowel disease
- Irritable bowel syndrome
- Ischemic bowel disease
- Obstruction
- Polyps
- Toxic megacolon
- Esophagitis
- Gastroesophageal reflux disease
- Mallory-Weiss tear
- Motility disorders
- Strictures
- Varices
Food allergies and food sensitivities
- Gluten intolerance
- Lactose intolerance
- Nut allergies
- Gastritis
- Peptic ulcer disease
- Pyloric stenosis
- Acute/chronic hepatitis
- Cirrhosis
Ingestion of toxic substances or foreign bodies
- G6PD deficiency
- Paget disease
- Phenylketonuria
- Rickets
Nutritional and vitamin disorders
- Hypervitaminosis/hypovitaminosis
- Obesity
- Acute/chronic pancreatitis
Small intestine disorders
- Appendicitis
- Celiac disease
- Intussusception
- Obstruction
- Polyps
- Incontinence
- Overactive bladder
- Prolapse
Congenital and acquired abnormalities
- Cryptorchidism
- Peyronie disease
- Trauma
- Vesicoureteral reflux
- Cystitis
- Epididymitis
- Orchitis
- Prostatitis
- Pyelonephritis
- Urethritis
- Bladder cancer
- Penile cancer
- Prostate cancer
- Testicular cancer
- Erectile dysfunction
- Hypospadias/epispadias
- Paraphimosis/phimosis
- Benign prostatic hyperplasia
- Hydrocele/varicocele
- Testicular torsion
- Clotting factor disorders
- Thrombocytopenias
- Polycythemia
- Thrombocytosis
- Hemochromatosis
- Sickle cell disease
- Thalassemia
- Transfusion reaction
Neoplasms, premalignancies, and malignancies
- Acute/chronic lymphocytic leukemia
- Acute/chronic myelogenous leukemia
- Lymphoma
- Multiple myeloma
- Myelodysplasia
- Botulism
- Campylobacter jejuni infection
- Chlamydia
- Cholera
- Diphtheria
- Gonococcal infections
- Gonorrhea
- Methicillin-resistant Staphylococcus aureus infection
- Rheumatic fever
- Rocky Mountain spotted fever
- Salmonellosis
- Shigellosis
- Tetanus
- Candidiasis
- Cryptococcosis
- Histoplasmosis
- Pneumocystis
- Atypical mycobacterial disease
- Tuberculosis
- Helminth infestations
- Malaria
- Pinworms
- Toxoplasmosis
- Trichomoniasis
Prenatal transmission of disorders
- Congenital varicella
- Herpes simplex virus
- Human papillomavirus
- Zika virus
Sepsis/systemic inflammatory response syndrome
- Cytomegalovirus infections
- Epstein-Barr virus infections
- Erythema infectiosum
- Herpes simplex virus infections
- HIV infection
- Human papillomavirus infections
- Influenza
- Measles
- Mumps
- Rabies
- Roseola
- Rubella
- Varicella-zoster virus infections
- Osteomyelitis
- Septic arthritis
Lower extremity disorders
- Avascular necrosis
- Developmental dysplasia
- Fractures/dislocations
- Osgood-Schlatter disease
- Slipped capital femoral epiphysis
- Soft-tissue injuries
- Fibromyalgia
- Gout/pseudogout
- Juvenile rheumatoid arthritis
- Osteoporosis
- Polyarteritis nodosa
- Polymyalgia rheumatica
- Polymyositis
- Reactive arthritis
- Rheumatoid arthritis
- Sjögren syndrome
- Systemic lupus erythematosus
- Systemic sclerosis (Scleroderma)
- Ankylosing spondylitis
- Cauda equina syndrome
- Herniated nucleus pulposus
- Kyphosis
- Scoliosis
- Spinal stenosis
- Sprain/strain
- Thoracic outlet syndrome
- Torticollis
- Trauma
Upper extremity disorders
- Fractures/dislocations
- Soft-tissue injuries
Closed head injuries
- Concussion
- Postconcussion syndrome
- Traumatic brain injury
Cranial nerve palsies
- Cluster headache
- Migraine
- Tension headache
- Encephalitis
- Meningitis
- Essential tremor
- Huntington disease
- Parkinson disease
- Tourette disorder
- Delirium
- Major/mild neurocognitive disorders
- Cerebral palsy
- Multiple sclerosis
- Myasthenia gravis
Peripheral nerve disorders
- Carpal tunnel syndrome
- Complex regional pain syndrome
- Guillain-Barré syndrome
- Peripheral neuropathy
- Focal seizures
- Generalized seizures
- Status epilepticus
- Arteriovenous malformation
- Cerebral aneurysm
- Intracranial hemorrhage
- Stroke
- Syncope
- Transient ischemic attack
Abuse and neglect
- Child abuse
- Domestic violence
- Elder abuse
- Sexual abuse
- Generalized anxiety disorder
- Panic disorder
- Phobias
Bipolar and related disorders
- Major depressive disorder
- Persistent depressive disorder (dysthymia)
- Premenstrual dysphoric disorder
- Suicidal/homicidal behaviors
Disruptive, impulse-control, and conduct disorders
- Conduct disorder
Feeding and eating disorders
Obsessive-compulsive and related disorders
- Attention-deficit/hyperactivity disorder
- Autism spectrum disorder
Schizophrenia spectrum and other psychotic disorders
- Narcolepsy
- Parasomnias
Somatic symptom and related disorders
Substance-related and addictive disorders
Trauma- and stressor-related disorders
- Adjustment disorders
- Post-traumatic stress disorder
Chronic obstructive pulmonary diseases
- Chronic bronchitis
- Emphysema
- Acute bronchiolitis
- Acute bronchitis
- Acute epiglottitis
- Croup
- Influenza
- Pertussis
- Pneumonias
- Bacterial
- Fungal
- HIV-related
- Viral
- Carcinoid tumors
- Lung cancer
- Pulmonary nodules
- Pleural effusion
- Pneumothorax
- Cor pulmonale
- Pulmonary embolism
- Pulmonary hypertension
Restrictive pulmonary diseases
- Idiopathic pulmonary fibrosis
- Pneumoconiosis
- Sarcoidosis
Sleep apnea/Obesity hypoventilation syndrome
Other pulmonary disorders
- Acute respiratory distress syndrome
- Asthma
- Cystic fibrosis
- Foreign body aspiration
- Hyaline membrane disease
- Glomerulonephritis
- Nephrotic syndrome
- Pyelonephritis
Acute kidney injury (acute renal failure)
Chronic kidney disease
Congenital or structural renal disorders
- Horseshoe kidney
- Hydronephrosis
- Polycystic kidney disease
- Renal vascular disease
End-stage renal disease
Fluid and electrolyte disorders
- Acid-base disorders
- Dehydration
- Hyperkalemia/hypokalemia
- Hypervolemia
- Hyponatremia
- Renal cell carcinoma
- Wilms tumor
- Abscess
- Fibroadenoma
- Fibrocystic changes
- Galactorrhea
- Gynecomastia
- Mastitis
- Abortion
- Abruptio placentae
- Breech presentation
- Cesarean delivery
- Cord prolapse
- Dystocia
- Ectopic pregnancy
- Fetal distress
- Gestational diabetes
- Gestational trophoblastic disease
- Hypertension disorders in pregnancy
- Incompetent cervix
- Multiple gestation
- Placenta previa
- Postpartum hemorrhage
- Premature rupture of membranes
- Rh incompatibility
- Shoulder dystocia
Neoplasms of the breast and reproductive tract
- Cysts
- Polycystic ovarian syndrome
- Torsion
Sexually transmitted infections/Pelvic inflammatory disease
- Physical assault
- Sexual assault
- Trauma in pregnancy
- Normal labor/delivery
- Postnatal/postpartum care
- Preconception/prenatal care
- Endometriosis
- Leiomyoma
- Prolapse
- Cystocele
- Prolapse
- Rectocele
- Vaginitis
Categories % Allocation - Dilated
- Hypertrophic
- Restrictive
- Stress
- Atrial fibrillation
- Atrial flutter
- Atrial tachycardia
- Atrioventricular block
- Bradycardia
- Bundle branch block
- Idioventricular rhythm
- Junctional rhythms
- Premature contractions
- QT prolongation
- Sick sinus syndrome
- Sinus arrhythmia
- Torsades de pointes
- Ventricular fibrillation
- Ventricular tachycardia
Congenital heart disease
- Atrial septal defect
- Coarctation of aorta
- Patent ductus arteriosus
- Patent foramen ovale
- Tetralogy of Fallot
- Transposition of the great vessels
- Ventricular septal defect
Coronary artery disease
- Acute coronary syndrome
- Angina pectoris
- Non–ST-segment elevation myocardial infarction
- ST-segment elevation myocardial infarction
- Unstable angina
- Primary hypertension
- Secondary hypertension
- Hypertensive emergencies
- Orthostatic hypotension
- Vasovagal hypotension
- Cardiogenic
- Distributive
- Hypovolemic
- Obstructive
Traumatic, infectious, and inflammatory heart conditions
- Cardiac tamponade
- Infective endocarditis
- Infective endocarditis
- Pericardial effusion
- Infective endocarditis
- Aortic aneurysm/dissection
- Arterial embolism/thrombosis
- Arteriovenous malformation
- Deep venous thrombosis
- Giant cell arteritis
- Peripheral artery disease
- Phlebitis/thrombophlebitis
- Varicose veins
- Venous insufficiency
- Acne vulgaris
- Folliculitis
- Perioral dermatitis
- Rosacea
- Erythema multiforme
- Stevens-Johnson syndrome
- Toxic epidermal necrolysis
Diseases/disorders of the hair and nails
- Alopecia
- Onychomycosis
- Paronychia/felon
Envenomations and arthropod bite reactions
- Bacterial
- Cellulitis
- Erysipelas
- Impetigo
- Candidiasis
- Dermatophyte infections
- Lice
- Scabies
- Condyloma acuminatum
- Exanthems
- Hand-foot-and-mouth disease
- Herpes simplex
- Molluscum contagiosum
- Varicella-zoster virus infections
- Verrucae
- Actinic keratosis
- Seborrheic keratosis
- Benign
- Malignant
- Premalignant
- Atopic dermatitis
- Contact dermatitis
- Drug eruptions
- Eczema
- Lichen planus
- Pityriasis rosea
- Psoriasis
- Atopic dermatitis
- Burns
- Lacerations
- Pressure ulcers
- Cherry angioma
- Hemangioma
- Purpura
- Purpura
- Telangiectasia
Other dermatologic disorders
- Acanthosis nigricans
- Hidradenitis suppurativa
- Lipomas/epidermal inclusion cysts
- Photosensitivity reactions
- Pilonidal disease
- Urticaria
- Cushing syndrome
- Pheochromocytoma
- Pheochromocytoma
- Multiple endocrine neoplasia
- Neoplastic syndrome
- Primary endocrine malignancy
- Hyperparathyroidism
- Hypoparathyroidism
- Acromegaly/gigantism
- Cushing disease
- Diabetes insipidus
- Dwarfism
- Pituitary adenoma
- Prolactinoma
- SIADH
- Goiter
- Hyperthyroidism
- Hypothyroidism
- Thyroid nodules
- Thyroiditis
- Conjunctivitis
- Corneal disorders
- Cataract
- Corneal ulcer
- Infectious
- Keratitis
- Pterygium
- Iritis
- Scleritis
- Uveitis
- Dacryoadenitis
- Dacryocystitis
- Dacryostenosis
- Keratoconjunctivitis sicca
- Blepharitis
- Chalazion
- Ectropion
- Entropion
- Hordeolum
- Nystagmus
- Optic neuritis
- Papilledema
- Orbital cellulitis
- Periorbital cellulitis
- Macular degeneration
- Retinal detachment
- Retinopathy
- Amaurosis fugax
- Amblyopia
- Glaucoma
- Strabismus
- Presbyopia
Ear disorders
- External ear
- Cerumen impaction
- Otitis externa
- Acoustic neuroma
- Dysfunction of eustachian tube
- Labyrinthitis
- Vertigo
- Cholesteatoma
- Otitis media
- Otosclerosis
- Tympanic membrane perforation
- Conductive
- Sensorineural
Other abnormalities of the ear
- Mastoiditis
- Meniere disease
- Tinnitus
Foreign bodies of the eyes, ears, nose, and throat
Trauma of the eyes, ears, nose, and throat
- Barotrauma of the ear
- Blowout fracture
- Corneal abrasion
- Globe rupture
- Hyphema
- Epistaxis
- Nasal polyps
- Rhinitis
- Sinusitis
- Infectious/inflammatory disorders
- Angioedema
- Aphthous ulcers
- Candidiasis
- Deep neck infection
- Dental abscess
- Dental caries
- Epiglottitis
- Gingivitis
- Laryngitis
- Peritonsillar abscess
- Pharyngitis
- Parotitis
- Sialadenitis
- Leukoplakia
- Acute/chronic cholecystitis
- Chronic cholecystitis
- Cholangitis
- Cholelithiasis
- Abscess/fistula
- Anal fissure
- Constipation
- Diverticulitis
- Fecal impaction/incontinence
- Hemorrhoids
- Inflammatory bowel disease
- Irritable bowel syndrome
- Ischemic bowel disease
- Obstruction
- Polyps
- Rectal prolapse
- Toxic megacolon
- Esophagitis
- Gastroesophageal reflux disease
- Mallory-Weiss tear
- Motility disorders
- Strictures
- Varices
- Zenker diverticulum
- Gastritis
- Gastroparesis
- Peptic ulcer disease
- Pyloric stenosis
- Acute/chronic hepatitis
- Chronic hepatitis
- Cirrhosis
- Fatty liver
- Portal hypertension
Ingestion of toxic substances or foreign bodies
- Phenylketonuria
- Rickets
- Food allergies and food sensitivities Hypervitaminosis/hypovitaminosis
- Malabsorption
- Refeeding syndrome
Pancreatic disorders
- Acute pancreatitis
- chronic pancreatitis
Small intestine disorders
- Appendicitis
- Celiac disease
- Intussusception
- Obstruction
- Polyps
Benign prostatic hyperplasia
- Incontinence
- Overactive bladder
- Prolapse
Congenital and acquired abnormalities
- Cryptorchidism
- Peyronie disease
- Trauma
- Vesicoureteral reflux
- Cystitis
- Epididymitis
- Orchitis
- Prostatitis
- Pyelonephritis
- Urethritis
- Bladder
- Penile
- Prostate
- Testicular
- Erectile dysfunction
- Hypospadias/epispadias
- Paraphimosis/phimosis
- Priapism
- Hydrocele/varicocele
- Testicular torsion
- Clotting factor disorders
- Thrombocytopenias
- Polycythemia
- Thrombocytosis
- G6PD deficiency
- Hemochromatosis
- Sickle cell disease
- Thalassemia
Neoplasms, premalignancies, and malignancies
- Acute/chronic lymphocytic leukemia
- Acute/chronic myelogenous leukemia
- Lymphoma
- Multiple myeloma
- Myelodysplasia
- Bartonella
- Botulism
- Campylobacter jejuni infection
- Chancroid
- Chlamydia
- Cholera
- Clostridioides difficile infection
- Diphtheria
- Gonococcal infections
- Methicillin-resistant Staphylococcus aureus infections
- Rheumatic fever
- Rocky Mountain spotted fever
- Salmonellosis
- Shigellosis
- Tetanus
- Blastomycosis
- Candidiasis
- Coccidioidomycosis
- Cryptococcosis
- Histoplasmosis
- Pneumocystis
- Atypical mycobacterial disease
- Tuberculosis
- Amebiasis
- Giardiasis
- Helminth infestations
- Malaria
- Pinworms
- Toxoplasmosis
- Trichomoniasis
Prenatal transmission of disorders
- Congenital varicella
- Herpes simplex virus
- Human papillomavirus
- Zika virus
- Group B streptococcus
Sepsis/systemic inflammatory response syndrome
- Coronavirus infections
- Cytomegalovirus infections
- Epstein-Barr virus infections
- Erythema infectiosum
- Herpes simplex virus infections
- HIV infection
- Human papillomavirus infections
- Influenza
- Measles
- Mumps
- Polio
- Rabies
- Roseola
- Rubella
- Varicella-zoster virus infections
- Osteomyelitis
- Septic arthritis
Lower extremity disorders
- Avascular necrosis
- Developmental dysplasia
- Fractures/dislocations
- Osgood-Schlatter disease
- Slipped capital femoral epiphysis
- Soft-tissue injuries
- Benign
- Malignant
- Paget disease of bone
- Connective tissue diseases
- Fibromyalgia
- Gout/pseudogout
- Juvenile rheumatoid arthritis
- Osteoporosis
- Polyarteritis nodosa
- Polymyalgia rheumatica
- Polymyositis
- Reactive arthritis
- Rheumatoid arthritis
- Sjögren syndrome
- Systemic lupus erythematosus
- Systemic sclerosis (Scleroderma)
- Ankylosing spondylitis
- Herniated disk disease
- Kyphosis
- Scoliosis
- Spinal stenosis
- Spondylolisthesis
- Spondylolysis
- Sprain/strain
- Torticollis
- Trauma
Thoracic outlet syndrome
Upper extremity disorders
- Fractures/dislocations
- Soft-tissue injuries
- Arteriovenous malformation
- Cerebral aneurysm
- Coma
- Hydrocephalus
- Intracranial hemorrhage
- Stroke
- Syncope
- Transient ischemic attack
Closed head injuries
- Concussion
- Postconcussion syndrome
- Traumatic brain injury
Cranial nerve palsies
- Cluster headache
- Migraine
- Tension headache
- Encephalitis
- Meningitis
- Essential tremor
- Huntington disease
- Parkinson disease
- Restless legs syndrome
- Tourette disorder
- Tardive dyskinesia
- Complex regional pain syndrome
- Guillain-Barré syndrome
- Mononeuropathies
- Peripheral neuropathies
- Cognitive impairment
- Delirium
- Cerebral palsy
- Multiple sclerosis
- Myasthenia gravis
- Focal seizures
- Generalized seizures
- Status epilepticus
Spinal cord syndromes
- Cauda equina syndrome
- Epidural abscess
- Spinal cord injuries
Abuse and neglect
- Child abuse
- Elder abuse
- Intimate partner violence
- Physical abuse
- Psychological abuse
- Sexual abuse
- Generalized anxiety disorder
- Panic disorder
- Phobias
Bipolar and related disorders
- Major depressive disorder
- Persistent depressive disorder (dysthymia)
- Premenstrual dysphoric disorder
- Suicidal/homicidal behaviors
Disruptive, impulse-control, and conduct disorders
Feeding and eating disorders
Human sexuality and gender dysphoria
- Attention-deficit/hyperactivity disorder
- Autism spectrum disorder
Obsessive-compulsive and related disorders
Psychogenic nonepileptic seizure
Schizophrenia spectrum and other psychotic disorders
- Narcolepsy
- Parasomnias
Somatic symptom and related disorders
Substance-related and addictive disorders
Trauma- and stressor-related disorders
- Adjustment disorders
- Bereavement
- Post-traumatic stress disorder
Acute respiratory distress syndrome
Foreign body aspiration
Hyaline membrane disease
- Acute bronchiolitis
- Acute bronchitis
- Acute epiglottitis
- Croup
- Empyema
- Influenza
- Pertussis
- Pneumonias
- Bacterial
- Fungal
- HIV-related
- Viral
- Benign
- Malignant
- Carcinoid tumors
Obesity hypoventilation syndrome
Obstructive pulmonary diseases
- Asthma
- Chronic obstructive pulmonary disease
- Cystic fibrosis
- Cor pulmonale
- Pulmonary edema
- Pulmonary embolism
- Pulmonary hypertension
Restrictive pulmonary diseases
- Idiopathic pulmonary fibrosis
- Pneumoconiosis
- Sarcoidosis
Acute kidney injury and acute renal failure
- Intrinsic
- Prerenal
- Postrenal
Chronic kidney disease/end-stage renal disease
Congenital or structural renal disorders
- Horseshoe kidney
- Hydronephrosis
- Polycystic kidney disease
- Renal cell carcinoma
- Wilms tumor
- Abscess
- Fibroadenoma
- Fibrocystic changes
- Galactorrhea
- Gynecomastia
- Mastitis
Human sexuality and gender identity
Neoplasms of the breast and reproductive tract
- Cysts
- Polycystic ovarian syndrome
- Torsion
Pelvic inflammatory disease
- Abruptio placentae
- Breech presentation
- Cervical insufficiency
- Cesarean and operative delivery
- Classifications of abortion
- Ectopic pregnancy
- Fetal distress
- Gestational diabetes
- Gestational trophoblastic disease
- Hypertensive disorders of pregnancy
- Labor/delivery
- Multiple gestation
- Placenta previa Postnatal/postpartum care
- Postpartum hemorrhage
- Postpartum pituitary disorders
- Postpartum psychiatric disorders
- Preconception/prenatal care
- Prelabor rupture of membranes
- Rh incompatibility
- Shoulder dystocia
- Umbilical cord prolapse
Trauma in pregnany
- Physical
- psychological
- Sexual
- Endometriosis
- Leiomyoma
- Prolapse
- Bartholin gland cysts
- Cystocele
- Prolapse
- Rectocele
- Vaginitis
PANCE task categories
The task categories on the PANCE assess candidates’ knowledge and skills related to tasks PAs perform when treating patients. Below are the contents of each category and how each category is allocated on the exam:
Categories % Allocation - General physical examination components and techniques
- Pertinent historical information
- Risk factors for development of significant medical conditions
- Significant physical examination findings
- Signs and symptoms of significant medical conditions
- Conducting comprehensive and/or problem-based interviews and physical examinations
- Eliciting patient information from other sources
- Identifying conditions requiring referral to or consultation with specialists
- Identifying pertinent patient and family historical information from patients and caregivers
- Identifying pertinent physical examination information
- Triaging of patients based on recognition of abnormal vital signs, examination findings, and/or general observations
- Appropriate patient education relating to diagnostic and laboratory studies
- Indications for initial and subsequent diagnostic and laboratory studies
- Indications for preventive screening tests
- Risks associated with diagnostic and laboratory studies
- Collecting diagnostic and laboratory specimens
- Communicating risks, benefits, and results effectively to other members of the healthcare team
- Communicating risks, benefits, and results effectively to patients, families, and caregivers
- Reviewing and interpreting results of diagnostic and laboratory studies, and correlating the results with history and physical examination findings
- Selecting appropriate diagnostic and/or laboratory studies
- Using diagnostic equipment safely and appropriately
- Significance of diagnostic and laboratory studies as they relate to diagnosis
- Significance of history as it relates to the differential diagnosis
- Significance of physical examination findings as they relate to diagnosis
- Developing multiple differential diagnoses for complicated and/or multisystem cases
- Formulating most likely differential diagnoses
- Incorporating history, physical examination findings, and diagnostic data into medical decision-making
- Recognizing the need for referral to a specialist
- Selecting the most likely diagnosis in light of presented data
- Appropriate patient education regarding preventable conditions and lifestyle modifications
- Early detection and prevention of medical conditions
- Effects of aging and changing family roles
- Genetic testing and counseling
- Human growth and development
- Human sexuality and gender identity, gender transition, and associated medical issues
- Immunization schedules and recommendations for infants, children, adults, and foreign travelers/adoptions
- Impact of patient demographics on risks for medical conditions
- Prevention of communicable diseases
- Preventive screening recommendations
- Psychosocial effects of illness, stress, and injury as well as related healthy coping strategies
- Signs of abuse and neglect
- Adapting health maintenance to an individual patient’s context
- Communicating effectively with and educating patients, family members, and caregivers regarding medical conditions
- Conducting education on modifiable risk factors with an emphasis on primary and secondary prevention
- Using counseling techniques
- Clinical procedures and their indications, contraindications, complications, risks, benefits, and techniques
- Conditions that constitute medical emergencies
- Criteria for admission to or discharge from the hospital or other facilities
- Management, treatment, and follow-up of medical conditions
- Palliative care and end-of-life issues
- Roles of other health professionals
- Sterile technique
- Therapeutic regimens
- Universal precautions and special isolation conditions
- Demonstrating technical expertise related to performing specific procedures
- Evaluating patient response to treatment/intervention
- Facilitating patient/caregiver adherence to and active participation in treatment
- Formulating and implementing treatment plans in accordance with applicable practice guidelines
- Interfacing in multidisciplinary teams, including education of other health care professionals
- Making appropriate dispositions
- Monitoring and managing nutritional status
- Prioritizing tasks
- Recognizing and initiating treatment for life-threatening conditions
- Using community resources to meet the needs of patients/caregivers
- Adverse effects, reactions, and toxicities
- Common alternative/complementary therapies and their interactions and toxicities
- Contraindications
- Drug interactions, including presentation and treatment
- Indications for use
- Mechanism of action
- Methods to reduce medication errors
- Monitoring and follow-up of pharmacologic regimens
- Presentation and treatment of allergic reactions
- Regulation of controlled substances
- Special populations requiring drug/dose modification
- Substances of abuse
- Assessing patient adherence to drug regimens
- Drafting a prescription
- Evaluating, treating, and reporting adverse drug reactions and/or adverse effects
- Identifying and managing medication misuse
- Interacting with pharmacists to address medication issues
- Maintaining knowledge of relevant pharmacologic agents
- Monitoring pharmacologic regimens and adjusting as appropriate
- Prescribing controlled substances appropriately
- Selecting appropriate pharmacologic therapy and dosing
- Basic biochemistry
- Basic genetics
- Human anatomy and physiology
- Microbiology
- Pathophysiology and immunology
- Evaluating emerging medical trends critically as they relate to patient care
- Maintaining awareness of trends in infectious disease
- Relating pathophysiologic principles to specific disease processes
- Cultural and religious beliefs related to health care
- Informed consent and refusal process
- Living will, advance directives, organ donation, code status, do not resuscitate, do not intubate, medical power of attorney, etc.
- Medicolegal issues
- Patient/provider rights and responsibilities
- Privacy, security, and responsibility related to medical record documentation and management
- Caring for patients with cognitive impairment
- Billing/coding to maintain accuracy and completeness for reimbursement and administrative purposes
- Demonstrating appropriate medical record documentation
- Using appropriate medical informatics sources
Patient care and communication (individual patients)
- Affordable and effective health care that is patient specific
- Cultural and religious diversity
- Stewardship of patient and community resources
- Acknowledging and applying patient/provider rights and responsibilities
- Ensuring patient satisfaction
- Providing patient advice and education regarding the informed consent and refusal process
- Providing patient advice and education related to end-of-life decisions
- Professional and clinical limitations, scope of practice, etc.
- Supervision parameters: malpractice, mandated reporting, conflict of interest, impaired provider, ethical principles
- Communicating and consulting with the supervising physician and/or other specialists/consultants
- Continuing medical education resources
- Critically analyzing evidence-based medicine
- Identifying and interpreting data from medical informatics sources and identifying appropriate reference sources
- Using epidemiologic techniques to evaluate the spread of disease
Public health (population/society)
- Basic disaster preparedness
- Infection control measures and response to outbreaks
- Occupational health issues as they pertain to health care as well as non–health care workers
- Population health, travel health, and epidemiology of disease states
- Protecting vulnerable populations and recognizing disparities in provision of and access to health care
- Quality improvement and patient safety
- Resource stewardship
- Ensuring patient safety and avoiding medical errors
Categories % Allocation - General physical examination components and techniques
- Pertinent historical information
- Risk factors for development of significant medical conditions
- Significant physical examination findings
- Signs and symptoms of significant medical conditions
- Reviewing pertinent resources to conduct comprehensive and/or problem-based interviews and physical examinations with compassion and empathy
- Identifying pertinent patient and family historical information from patients and caregivers
- Identifying pertinent physical examination information
- Triaging of patients based on recognition of abnormal vital signs, examination findings, and/or general observations
- Patient-centered education relating to diagnostic and laboratory studies
- Indications for initial and subsequent diagnostic and laboratory studies
- Indications for preventive screening tests
- Collecting diagnostic and laboratory specimens
- Communicating risks, benefits, and results effectively to other members of the healthcare team
- Communicating risks, benefits, and results effectively to patients, families, and caregivers
- Integrating diagnostic and laboratory results with history and physical examination findings
- Reviewing and interpreting results of diagnostic and laboratory studies
- Selecting appropriate diagnostic and laboratory studies
- Using diagnostic equipment safely and appropriately
- Significance of diagnostic and laboratory studies as they relate to diagnosis
- Significance of history as it relates to the differential diagnosis
- Significance of physical examination findings as they relate to diagnosis
- Formulating most likely differential diagnoses
- Incorporating history, physical examination findings, and diagnostic data into medical decision-making
- Recognizing the need for referral to a specialist
- Selecting the most likely diagnosis in light of presented data
- Appropriate patient education regarding preventable conditions and lifestyle modifications
- Early detection and prevention of medical conditions
- Effects of aging and changing family roles
- Human growth and development
- Human sexuality and gender identity, gender transition, and associated medical issues
- Immunization schedules and recommendations for infants, children, adults, and foreign travelers/adoptions
- Impact of patient demographics on risks for medical conditions
- Prevention of communicable diseases
- Preventive screening recommendations
- Psychosocial effects of illness, stress, and injury as well as related healthy coping strategies
- Signs of abuse and neglect
- Adapting health maintenance to an individual patient’s context
- Communicating effectively with and educating patients, family members, and caregivers regarding medical conditions
- Conducting education on modifiable risk factors with an emphasis on primary and secondary prevention
- Reporting suspected abuse and/or trafficking
- Using appropriate screening tools
- Using counseling techniques
- Clinical procedures and their indications, contraindications, complications, risks, benefits, and techniques
- Conditions that constitute medical emergencies
- Criteria for admission to or discharge from the hospital or other facilities
- Management, treatment, and follow-up of medical conditions
- Palliative care and end-of-life issues
- Roles of other health professionals
- Sterile technique
- Support structure systems, based on patient needs
- Therapeutic regimens
- Universal precautions and special isolation conditions
- Demonstrating technical expertise related to performing specific procedures
- Determining the existence of support structures and using community resources to meet the needs of patients and caregivers
- Evaluating patient competence to make decisions
- Evaluating patient response to treatment/intervention
- Facilitating patient/caregiver adherence to and active participation in treatment
- Formulating and implementing treatment plans in accordance with applicable practice guidelines
- Interfacing in multidisciplinary teams, including education of other health care professionals
- Making appropriate dispositions
- Monitoring and managing nutritional status
- Prioritizing tasks
- Recognizing and initiating treatment for life-threatening conditions
- Using community resources to meet the needs of patients/caregivers
- Alternative/complementary therapies and their side effects, interactions, and toxicities
- Contraindications
- Drug interactions, including presentation and treatment
- Indications for use
- Mechanism of action
- Methods to reduce medication errors
- Monitoring and follow-up of pharmacologic regimens
- Pharmacokinetics, pharmacogenomics, and pharmacodynamics
- Prescribing, monitoring, and regulating controlled substances
- Presentation and management of adverse effects, allergic reactions and toxicities
- Special populations requiring drug/dose modification
- Substances of abuse
- Assessing patient adherence to drug regimens
- Drafting a prescription
- Evaluating, treating, and reporting adverse drug reactions and/or adverse effects
- Identifying and managing medication misuse
- Interacting with pharmacists to address medication issues
- Maintaining knowledge of relevant pharmacologic agents
- Monitoring pharmacologic regimens and adjusting as appropriate
- Prescribing controlled substances appropriately
- Selecting appropriate pharmacologic therapy and dosing
- Genetics
- Human anatomy and physiology
- Microbiology
- Pathophysiology
- Immunology
- Pharmacology
- Human behavior (e.g., sociology, psychology)
- Evaluating emerging medical trends critically as they relate to patient care
- Maintaining awareness of trends in infectious disease
- Relating pathophysiologic principles to specific disease processes
- Incorporating evidence-based medicine practices
- Informed consent and refusal process
- Living will, advance directives, organ donation, code status (e.g., do not resuscitate, do not intubate), medical power of attorney
- Medicolegal issues
- Patient preferences related to health care (e.g., cultural, religious, gender)
- Patient/provider rights and responsibilities and termination of the patient-provider relationship, including against medical advice
- Privacy, security, and responsibility related to medical record documentation and management
- Caring for patients with cognitive impairment
- Billing/coding to maintain accuracy and completeness for reimbursement and administrative purposes
- Demonstrating appropriate medical record documentation
- Using appropriate medical informatics sources
Patient care and communication (individual patients)
- Affordable and effective health care that is patient-specific
- Communication and care preferences of diverse patient populations
- Impact of social determinants of health
- Acknowledging and applying patient/provider rights and responsibilities
- Establishing clinical rapport
- Patient-based interactions, including the ability to demonstrate cultural humility and competency
- Providing patient advice and education regarding the informed consent and refusal process
- Providing patient advice and education related to end-of-life decisions
PA role in professional practice
- Professional and clinical limitations, scope of practice, etc.
- Practice parameters: malpractice, mandated reporting, conflict of interest, impaired provider, ethical principles, effects of implicit bias
- Communicating and consulting with members of the health care team
- Continuing medical education resources
- Critically analyzing evidence-based medicine
- Identifying and interpreting data from medical informatics sources and identifying appropriate reference sources
Public health (population/society)
- Basic disaster preparedness
- Infection control measures and response to outbreaks
- Occupational health issues as they pertain to health care as well as non–healthcare workers
- Population health, travel health, and epidemiology of disease states
- Protecting vulnerable populations and recognizing disparities in the provision of and access to healthcare
- Accountability
- Effective resource management and utilization
- Quality improvement and patient safety
- Ensuring patient safety and avoiding medical errors

How medical content and task categories are tested
As you might have noticed, the percent allocation on each table equals 100%. This is because the medical content questions are coded to task areas (with the exception of the “Professional Practice” task category, totaling 5% allocation). As a result, medical content makes up 95% of the exam. Additionally, up to 20% of tested content may be related to general surgical topics. This percent allocation varies by exam.
PANCE Practice Questions Based on the NCCPA Blueprint
The UWorld PA QBank is written by practicing physician assistants to put aspiring PAs on a path to success. Our PANCE sample questions and industry-leading rationales are based on the latest NCCPA blueprints to ensure you know everything you’re expected to know on exam day. To see how our active-learning methodology can help you achieve PANCE success, try our example problems below. Submit your answers to view our award-winning explanations.
- Cardiovascular System
- Hematologic System
- Musculoskeletal System
A 1-month-old boy is brought to the office for a routine visit. His prenatal and birth histories are unremarkable. His vital signs and pulse oximetry are normal. Examination shows a harsh, 3/6 holosystolic murmur over the left lower sternal border. Palpation indicates no thrill over the precordial region. Brachial and femoral pulses are 2+ and equal. The skin is pink and well perfused. ECG is normal. Which of the following is the best next step in management of this patient?
- Digoxin and diuretic therapy
- Echocardiography
- Oxygen administration
- Prostaglandin E1 therapy
- Reassurance and no further workup

This patient’s holosystolic murmur at the left lower sternal border is characteristic of a ventricular septal defect (VSD). VSD is the most common cause (~25%) of congenital heart disease. The presence of a harsh and loud murmur and a normal ECG, and the absence of concerning symptoms (eg, tachycardia, tachypnea, failure to thrive, right ventricular heave) make a small VSD more likely. Echocardiography should be performed to determine the location and size of the defect and to rule out other defects.
Small VSDs close spontaneously in 75% of children by age 2 years with no long-term sequelae. Large defects often present with a softer murmur due to less turbulence across a larger defect. High-volume shunting across the defect leads to pulmonary overcirculation, pulmonary hypertension, growth failure, congestive heart failure, and Eisenmenger syndrome.
(Choice A and C) This patient has no evidence of heart failure or hypoxia and therefore does not require digoxin, diuretics, or oxygen.
(Choice D) Prostaglandin E1 therapy is used to keep the ductus arteriosus open in infants with congenital heart defects that depend on blood flow between the systemic and pulmonary circulations through the ductus (eg, D-transposition of the great arteries with an intact atrioventricular septum).
(Choice E) No workup is needed if the murmur sounds like an innocent “flow” murmur of childhood, which is typically a grade 1 or 2 midsystolic ejection murmur.
Educational objective:
The classic ventricular septal defect murmur is a harsh, holosystolic murmur best heard at the left lower sternal border. Echocardiography should be performed to determine the location and size of the defect and to rule out other defects. Most small ventricular septal defects close spontaneously and require no treatment.A 78-year-old resident of an extended care facility is brought to the emergency department due to lethargy, fevers, and poor oral intake for the last day. Temperature is 39 C (102 F), blood pressure is 70/40 mm Hg, and pulse is 120/min and regular. On examination, the patient is lethargic but arousable. His extremities are warm. A Foley catheter is inserted into the bladder and drains 500 mL of cloudy urine consistent with urinary tract infection. Five hours after admission, the patient begins to bleed from the nose and venipuncture sites, and the Foley catheter begins to drain blood-tinged urine. Which of the following laboratory findings would most likely to be seen in this patient?
- Increased fibrinogen
- Normal D-dimer
- Normal partial thromboplastin time
- Normal prothrombin time
- Thrombocytopenia
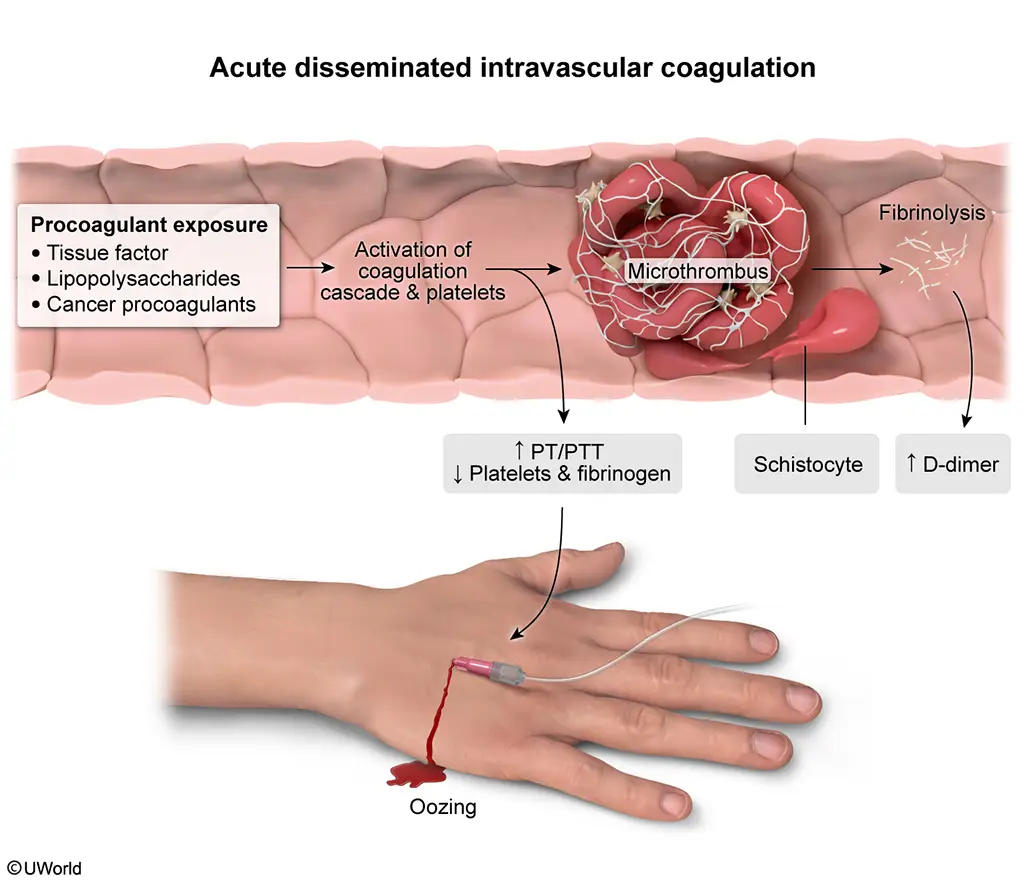
This elderly patient with fever, urinary retention, and cloudy urine likely has a urinary tract infection complicated by sepsis (eg, hypotension, tachycardia). The subsequent development of venipuncture site and urinary tract bleeding indicates likely progression to disseminated intravascular coagulation (DIC). DIC is a common complication of sepsis with gram-negative pathogens (eg, urinary tract organisms) because the bacteria can trigger the coagulation cascade, leading to the following:
- The formation of fibrin- and platelet-rich thrombi in the microvasculature, which consumes coagulation factors, resulting in prolonged PT/PTT (Choices C and D). The formation of the thrombi also leads to decreased fibrinogen (Choice A) and decreased platelets (thrombocytopenia)
- Subsequent fibrinolysis to clear the thrombi, which generates and increases D-dimer (a fibrin degradation product) (Choice B)
- The consumption of anticoagulation proteins (eg, protein C/S)
Manifestations of acute DIC usually include mucocutaneous bleeding, oozing from venipuncture sites, ecchymosis, and petechiae due to lack of coagulation factors, fibrinogen, and platelets. Organ dysfunction (eg, renal insufficiency, pulmonary damage) also commonly occurs.
Educational objective:
Disseminated intravascular coagulation (DIC) typically presents with signs of bleeding (eg, oozing from venipuncture sites) in the setting of sepsis, malignancy, or severe trauma. Widespread activation of the coagulation cascade leads to the formation of intravascular microthrombi, which consumes coagulation factors (prolonged PT/PTT), platelets (thrombocytopenia), and fibrinogen. Subsequent fibrinolysis increases D-dimer.A 45-year-old woman comes to the emergency department for acute onset of low back pain radiating down her left leg after lifting heavy boxes at home. She has had no muscle weakness and has no concerns with bowel or bladder function. The back pain worsens with coughing or bearing down. Neurologic examination reveals 5/5 muscle strength in all 4 extremities with 2+ reflexes. Straight-leg raise sign is positive on the left. Sensory examination reveals reduced pinprick and temperature sensation along the posterolateral region of the left leg. X-ray of the lumbar spine reveals only degenerative changes. Which of the following is the best next step in management of this patient?
- Bone density testing
- Gabapentin and tramadol
- Light exercise and a nonsteroidal anti-inflammatory drug
- MRI of the lumbar
- Physical therapy
- Maintain moderate activity
- NSAIDs or acetaminophen
- Consider: muscle relaxants, spinal manipulation
- Intermittent use of NSAIDs or acetaminophen
- Exercise therapy (stretching/strengthening, aerobic)
- Consider: tricyclic antidepressants, duloxetine
- Exercise therapy
- Education
This patient’s back pain that radiates down the leg and is worsened with coughing or bearing down is likely due to acute lumbosacral radiculopathy (ALSR). ALSR is most often due to a mechanical compression of the L5 and/or S1 dorsal root (eg, herniated disc). Patients typically have low back and leg pain (sciatica), often with associated numbness and/or weakness in the leg. Reproduction of radicular pain with flexion at the hip and dorsiflexion at the ankle (ie, positive straight-leg raise) is relatively specific for the diagnosis.
Most patients have spontaneous improvement and can be managed conservatively with nonsteroidal anti-inflammatory drugs (NSAIDs) and maintaining light-normal activity. A brief period of bed rest (
